A study in patients with SMA showed SPINRAZA® (nusinersen)
Achieved meaningful results across
age
groups—from infants to
adults1-3
Backed by the longest clinical trial
program to date in infants and
children.4 Supported by extensive
real-world evidence in
adults, teens,
and older children2,3,5
Click the tabs to see the data in the selected population
SPINRAZA for LATER-ONSET SMA
CHERISH
The first clinical trial in later-onset SMA with proven results1,6
Pivotal trial: CHERISH1,8
Study overview: A phase 3, multicenter, randomized (2:1), double-blind, sham procedure–controlled trial of the Low Dose Regimen (12 mg loading doses/12 mg maintenance doses)
Study duration: 15 months
Participants: 126 patients with later-onset SMA, aged 2 to 9 years at screening, who had not achieved independent walking
Primary outcome measured: Least-squares mean change from baseline in the HFMSE score at 15 months of treatment
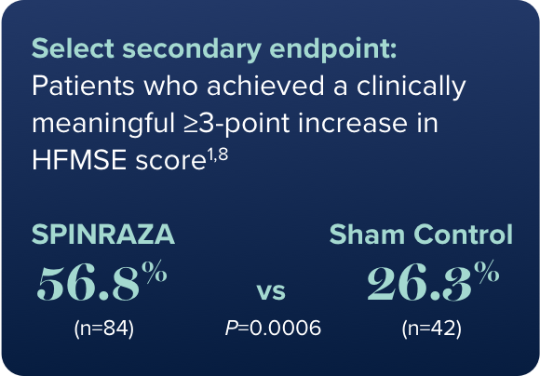
Select secondary outcomes measured: Clinically meaningful change in HFMSE score ≥3 points and change in upper limb function as measured by RULM
Study limitations: Differences in dosing compared with the approved SPINRAZA schedule
Safety: The most common adverse reactions were fever (43%), headache (29%), vomiting (29%), and back pain (25%)
HFMSE, Hammersmith Functional Motor Scale—Expanded; RULM, Revised Upper Limb Module; SMA, spinal muscular atrophy.
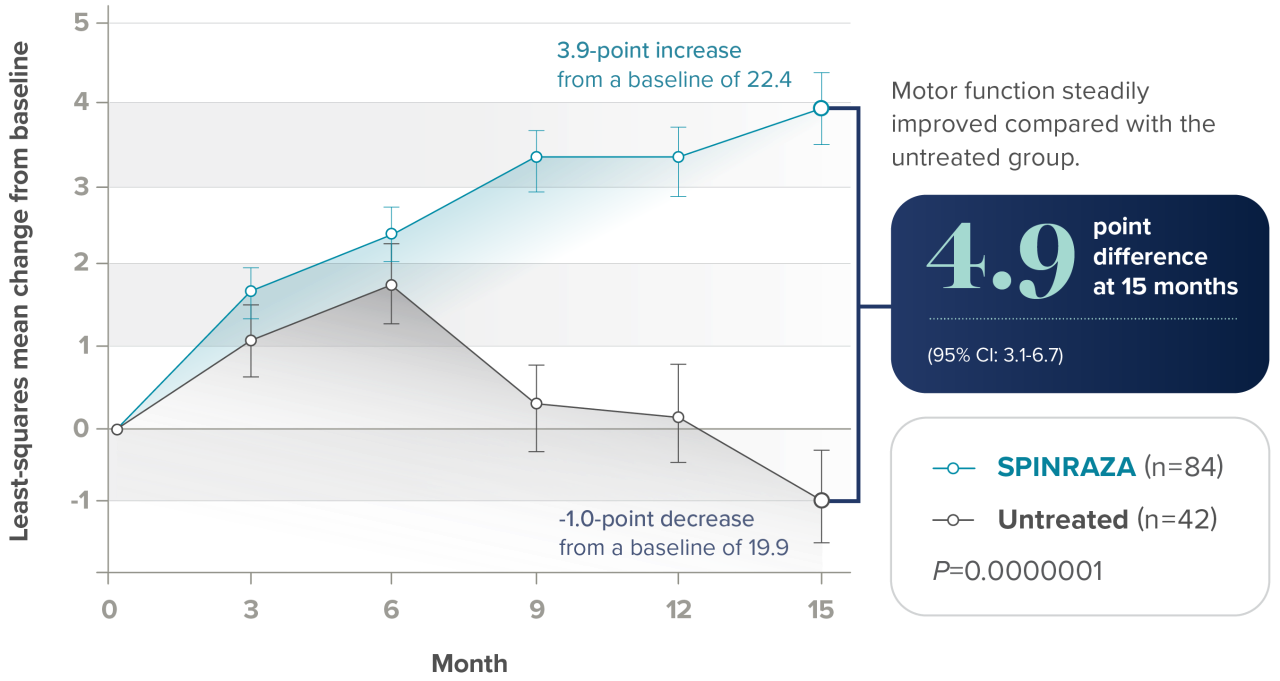
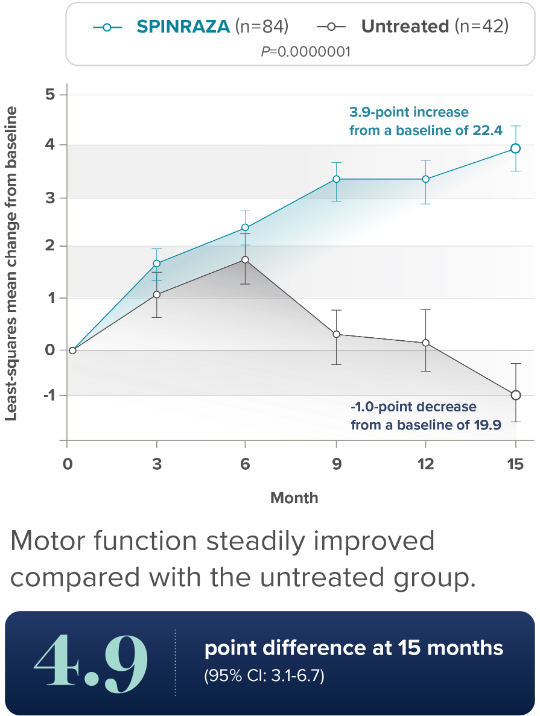
Significant improvements seen in overall motor function1,6
Primary endpoint: Least-squares mean change from baseline in HFMSE score at 15 months

Learn more about the mobility measures used in the SPINRAZA clinical trials.
Secondary outcome: Least-squares mean change from baseline in upper limb function score at 15 months


CI, confidence interval.